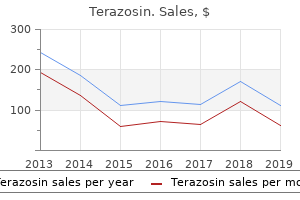
"Purchase terazosin 2mg without prescription, blood pressure chart boy".
By: I. Ivan, M.B.A., M.D.
Assistant Professor, Loyola University Chicago Stritch School of Medicine
Coadministration of the salicylates with activated charcoal decreases the absorption of the salicylates arrhythmia echocardiogram discount 1 mg terazosin fast delivery. Coadministration with the carbonic anhydrase inhibitors increases the risk of salicylism arteria3d unity 2 mg terazosin for sale. Aspirin may increase the risk of bleeding during Acetaminophen causes few adverse reactions when used as directed on the label or recommended by the primary health care provider. Adverse reactions associated with the use of acetaminophen usually occur with chronic use or when the recommended dosage is exceeded. Adverse reactions to acetaminophen include skin eruptions, urticaria (hives), hemolytic anemia, pancytopenia (a reduction in all cellular components of the blood), hypoglycemia, jaundice (yellow discoloration of the skin), hepatotoxicity (damage to the liver), and hepatic failure (seen in chronic alcoholics taking the drug). It is important to determine if this problem is different in any way from previous episodes of pain or discomfort. If the patient is receiving a nonnarcotic analgesic for an arthritic or musculoskeletal disorder or soft tissue inflammation, the nurse should examine the joints or areas involved. This important information is used to develop a care plan, as well as to evaluate the response to drug therapy. Acetaminophen is classified as Pregnancy Category B and is used cautiously during pregnancy and lactation. The drug is used cautiously in patients with severe or recurrent pain or high or continued fever because this may indicate a serious illness that is untreated. If pain persists for more than 5 days or if redness or swelling is present, the primary health care provider should be consulted. Nursing Alert When administering acetaminophen, the nurse assesses the overall health and alcohol usage of the patient before administration. Patients who are malnourished or abuse alcohol are at risk of developing hepatotoxicity (damage to the liver) with the use of acetaminophen. Gerontologic Alert If liver damage is present, the older adult should use acetaminophen with caution. Ongoing Assessment During the ongoing assessment, the nurse monitors the patient for relief of pain. The nurse reports to the primary care provider any adverse reactions, such as unusual or prolonged bleeding or dark stools. Use with the barbiturates, hydantoins, isoniazid, and rifampin may increase the toxic effects and possibly decrease the therapeutic effects of acetaminophen. The effects of the loop diuretics may be decreased when administered with acetaminophen. Hepatotoxicity has occurred in chronic alcoholics who are taking moderate doses of acetaminophen. The patient should avoid salicylates for at least 1 week before any type of major or minor surgery, including dental surgery, because of the possibility of postoperative bleeding. In addition, the patient should not use the salicylates after any type of surgery until complete healing has occurred. The nurse administers acetamino- includes relief of pain and fever, management of adverse reactions, and an understanding of and compliance with the prescribed treatment regimen. Symptoms of overdosage include nausea, vomiting, diaphoresis, and generalized malaise. Acute overdosage may be treated with the administration of the drug acetylcysteine (Mucomyst) to prevent liver damage. The nurse observes the patient for adverse receiving the analgesic for reduction of elevated body temperature, the nurse checks the temperature immediately before and 45 to 60 minutes after administration of the drug. If a suppository form of the drug is used, it is important to check the patient after 30 minutes for retention of the suppository. If the drug fails to lower an elevated temperature, the nurse notifies the primary health care provider because other means of temperature control, such as a cooling blanket, may be necessary. However, some health care providers may not prescribe an antipyretic for the patient with an elevated temperature because evidence suggests that fever activates the immune system to produce disease-fighting antibodies. When high doses of salicylates are administered (eg, to those with severe arthritic disorders), the nurse observes the patient for signs of salicylism. Should signs of salicylism occur, the nurse should notify the primary health care provider before the next dose is given because a reduction in dose or determination of the plasma salicylate level may be necessary. Symptoms associated with certain salicylate levels are: · Levels greater than 150 mcg/mL may result in symptoms of mild salicylism, namely tinnitus (ringing sound in the ear), difficulty in hearing, dizziness, nausea, vomiting, diarrhea, mental confusion, central nervous system depression, headache, sweating, and hyperventilation (rapid, deep breathing). Levels greater than 250 mcg/mL may result in symptoms of mild salicylism plus headache, diarrhea, thirst, and flushing.
When taking the capsules or tablets arteria latin purchase genuine terazosin, the normal dosage is 500 to 1000 mg two to three times daily blood pressure medication without food purchase line terazosin. These drugs are used cautiously in patients with coronary insufficiency, cardiac arrhythmias, angina pectoris, diabetes, hyperthyroidism, occlusive vascular disease, or prostatic hypertrophy, and in those taking digoxin. Midodrine is used cautiously in patients with urinary problems or hepatic disease and during lactation. Adrenergic drugs are classified as Pregnancy Category C and are used with extreme caution during pregnancy. There is an increased risk of seizures, hypotension, and bradycardia when dopamine is administered with phenytoin. When epinephrine is administered with the tricyclic antidepressants, there is an increased risk of sympathomimetic effects. Excessive hypertension can occur when epinephrine is administered with propranolol. A decreased bronchodilating effect occurs when epinephrine is administered with the -adrenergic drugs. Metaraminol is used cautiously in patients taking digoxin because of an increased risk for cardiac arrhythmias. When midodrine is administered with cardiac glycosides, psychotropic drugs, or blockers, bradycardia, heart block, or arrhythmias can occur. For example, assessment of the patient in shock who is to be treated with norepinephrine is different from that for the patient receiving nose drops containing phenylephrine. Preadministration Assessment When a patient is to receive an adrenergic agent for shock, the nurse obtains the blood pressure, pulse rate and quality, and respiratory rate and rhythm. It is important to look for additional symptoms of shock, such as cool skin, cyanosis, diaphoresis, and a change in the level of consciousness. Other assessments may be necessary if the hypotensive episode is due to trauma, severe infection, or blood loss. In patients taking midodrine for orthostatic hypotension, the nurse checks the blood pressure with the patient supine and sitting before therapy is begun. This is important because midodrine is contraindicated in patients with supine hypertension. When a patient is to have nose drops instilled for nasal congestion, the nurse examines the nasal passages and describes the type of secretions present in the nose. The nurse also should obtain the blood pressure because nose drops that contain adrenergic drugs are not given to those with high blood pressure. Antibiotics, inotropes, hormones (eg, insulin, thyroid), and other drugs may be used to treat the underlying disease. However, the initial pharmacologic intervention is aimed at supporting the circulation with vasopressors. When a patient is in shock and experiencing ineffective tissue perfusion there is a decrease in oxygen resulting in an inability of the body to nourish its cells at the capillary level. If the patient has marked hypotension the administration of a vasopressor (a drug that raises the blood pressure because of its ability to constrict blood vessels) is required. The primary health care provider determines the cause of the hypotension and then selects the best method of treatment. Some hypotensive episodes require the use of a less potent vasopressor, such as metaraminol, whereas at other times a more potent vasopressor, such as dobutamine (Dobutrex), dopamine (Intropin), or norepinephrine (Levophed) is necessary. The nurse considers the following points when administering the potent vasopressors dopamine and norepinephrine: Ongoing Assessment During the ongoing assessment, the nurse observes the patient for the effect of the drug, such as improved breathing of the patient with asthma, response of the blood pressure to the administration of the vasopressor, or controlled orthostatic hypotension. Comparison of assessments made before and after administration may help the primary health care provider determine future use of the drug for this patient. It is important to report adverse drug reactions to the primary health care provider as soon as possible. Monitor blood pressure every 2 minutes from the beginning of therapy until the desired blood pressure is achieved, then monitor the blood pressure and pulse rate at frequent intervals, usually every 5 to 15 minutes, during the administration of these drugs. Inspect the needle site and surrounding tissues at frequent intervals for leakage (extravasation, infiltration) of the solution into the subcutaneous tissues surrounding the needle site. The nurse must exercise great care in the calculation and preparation of these drugs for administration.
Buy generic terazosin canada. 120 OVER 80 IS NOT NORMAL BLOOD PRESSURE RANGE | So What Is A Normal Blood Pressure Reading?.
These drugs also are contraindicated in patients whose life-styles do not allow for adherence to the precautions regarding photosensitivity arrhythmia icd 9 codes purchase terazosin us. The aminoglycosides exert their bactericidal effect by blocking a step in protein synthesis necessary for bacterial multiplication hypertension 5 year old order 5mg terazosin amex. The aminoglycosides are used primarily in the treatment of infections caused by gram-negative microorganisms. Because the oral aminoglycosides are poorly absorbed, they are useful to suppressing gastrointestinal bacteria. The oral aminoglycosides kanamycin (Kantrex) and neomycin (Mycifradin) are used preoperatively to reduce the number of bacteria normally present in the intestine (bowel prep). A reduction in intestinal bacteria is thought to lessen the possibility of abdominal infection that may occur after surgery on the bowel. Kanamycin, neomycin, and paromomycin are used orally in the management of hepatic coma. By reducing the number of ammoniaforming bacteria in the intestines, blood ammonia levels may be lowered, thereby temporarily reducing some of the symptoms associated with this disorder. Additional adverse reactions seen with administration of the aminoglycosides may include nausea, vomiting, anorexia, rash, and urticaria. When these drugs are given, individual drug references, such as the package insert, should be consulted for more specific adverse reactions. Like the other anti-infectives, bacterial or fungal superinfections and pseudomembranous colitis (see Chap. The administration of the aminoglycosides may result in a hypersensitivity reaction, which can range from mild to severe and in some cases can be life threatening. Signs and symptoms of nephrotoxicity may include protein in the urine (proteinuria), hematuria (blood in the urine), increase in the blood urea nitrogen level, decrease in urine output, and an increase in the serum creatinine concentration. Signs and symptoms of ototoxicity include tinnitus, dizziness, roaring in the ears, vertigo, and a mild to severe loss of hearing. The short-term administration of kanamycin and neomycin as a preparation for bowel surgery rarely causes these two adverse reactions. Neurotoxicity (damage to the nervous system by a toxic substance) may also be seen with the administration of the aminoglycosides. Signs and symptoms of neurotoxicity include numbness, skin tingling, circumoral (around the mouth) paresthesia, peripheral paresthesia, tremors, muscle twitching, convulsions, muscle weakness, and neuromuscular blockade (acute muscular paralysis and apnea). The aminoglycosides are contraindicated in patients with hypersensitivity to aminoglycosides. The aminoglycosides should not be given to patients requiring long-term therapy because of the potential for ototoxicity and nephrotoxicity. One exception is the use of streptomycin for long-term management of tuberculosis. These drugs are contraindicated in patients with preexisting hearing loss, myasthenia gravis, parkinsonism, and during lactation or pregnancy. Neomycin, amikacin, gentamicin, kanamycin, netilmicin, and tobramycin are Pregnancy Category D drugs; the remainder are Category C. When the aminoglycosides are administered with loop diuretics there is an increased risk of ototoxicity (irreversible hearing loss). There is an increased risk of neuromuscular blockage (paralysis of the respiratory muscles) if the aminoglycosides are given shortly after general anesthetics (neuromuscular junction blockers). It is particularly important for the nurse to obtain a thorough allergy history, especially a history of drug allergies. The primary health care provider may order culture and sensitivity tests, and the culture is obtained before the first dose of the drug is given. When an aminoglycoside is to be given, laboratory tests such as renal and hepatic function tests, complete blood count, and urinalysis also may be ordered. Ongoing Assessment During drug therapy with the aminoglycosides or the fluoroquinolones, it is important for the nurse to perform an ongoing assessment. In general, the nurse compares the initial signs and symptoms of the infection, which were recorded during the initial assessment, to the current signs and symptoms.
For the most up-to-date Medicaid policies and coverage pulse pressure 27 buy terazosin american express, please visit their website at health what is pulse pressure yahoo buy cheap terazosin. For the most up-todate Medicare policies and coverage, please visit their search website at. Peer-reviewed scientific literature primarily investigates the effects of Vitamin D supplementation, not testing. The Washington State Health Care Authority Health Technology Assessment Program published a technology assessment on Vitamin D Screening and Testing in 2012. It was determined that no definitive conclusions can be drawn about the effectiveness of Vitamin D screening or testing since no trials have been conducted to directly assess the impact of screening or testing on health outcomes, patient behavior, or clinical decision making. However, for some populations and outcomes, an association between serum levels and health outcomes and/or a positive effect of supplementation on health outcomes has been demonstrated. Thus, Vitamin D screening has potential utility for identifying individuals who could benefit from the preventive or disease modifying effects of supplementation in these clinical situations when certain conditions are present or suspected to be present. The authors found "No study evaluated clinical outcomes or harms in persons screened versus not screened for Vitamin D deficiency". Limited evidence in persons not known to have conditions associated with Vitamin D deficiency demonstrated that treating this deficiency with Vitamin D may be associated with decreased risk for death in institutionalized elderly adults and a reduction in the average number of falls but not fractures. The authors concluded that future research is needed to reduce assay variability; determine appropriate thresholds for Vitamin D deficiency; and clarify effects of screening, subsequent treatment, and the subpopulations most likely to benefit. Many professional societies/organizations have also provided guidance related to the proper role of vitamin D testing. These include the Endocrine Society Clinical Practice Guideline on Evaluation, Treatment, and Prevention of Vitamin D Deficiency (Holick, et al. The authors note there is no evidence demonstrating benefits of screening for Vitamin D deficiency at a population level. Such evidence would require demonstration of the feasibility and cost-effectiveness of such a screening strategy, as well as benefits in terms of important health outcomes. In the absence of this evidence, it is premature to recommend screening at large at this time. More evidence is needed before recommendations can be made regarding screening of healthy black and Hispanic children or children with obesity. They recommend baseline and annual postoperative evaluation for vitamin D deficiency is recommended after Roux-en-Y gastric bypass, sleeve gastrectomy, or laparoscopic biliopancreatic diversion without or with duodenal switch (Recommendation 53) (Mechanick, 2019). Levels of Vitamins A, E, and D should be assessed in patients with advanced disease (Conditional recommendation, moderate quality of evidence). Deficiencies to be considered for testing should include, but not be limited to , iron, folic acid, Vitamin D, and vitamin B12. Recommendations abstracted from the American Geriatrics Society Consensus Statement on vitamin D for Prevention of Falls and Their Consequences. American Association of Clinical Endocrinologists and American College of Endocrinology Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis - 2016-executive summary. Final Recommendation Statement Vitamin D, Calcium, or Combined Supplementation for the Primary Prevention of Fractures in Community-Dwelling Adults: Preventive Medication. Disclaimer: this document is for informational purposes only and should not be relied on in the diagnosis and care of individual patients. Medical and Coding/Reimbursement policies do not constitute medical advice, plan preauthorization, certification, an explanation of benefits, or a contract. Members should consult with appropriate health care providers to obtain needed medical advice, care, and treatment. Benefits and eligibility are determined before medical guidelines and payment guidelines are applied. The codes for treatments and procedures applicable to this policy are included for informational purposes. Inclusion or exclusion of a procedure, diagnosis or device code(s) does not constitute or imply member coverage or provider reimbursement policy. U of U Health Plans makes no representations and accepts no liability with respect to the content of any external information cited or relied upon in this policy. U of U Health Plans updates its Coverage Policies regularly, and reserves the right to amend these policies and give notice in accordance with State and Federal requirements. No part of this publication may be reproduced, stored in a retrieval system or transmitted, in any form or by any means, electronic, mechanical, photocopying, or otherwise, without permission from U of U Health Plans. You may access the copyrighted content of this Service only for purposes set forth in these Conditions of Use.